Evaluating modular reference models for early oncology economic evaluation
Economic modeling plays an increasingly significant role across the product lifecycle, supporting early value assessment, global cost-effectiveness evaluation, health technology assessment (HTA) submissions, and post-launch stakeholder engagement. In oncology, the need for early health economic assessment has intensified as manufacturers seek to inform evidence generation, pricing strategy, and payer engagement before mature Phase 3 trial data become available. However, early-stage oncology evidence often relies on single-arm studies, immature survival data, and rapidly evolving standards of care, creating challenges for traditional modeling approaches.
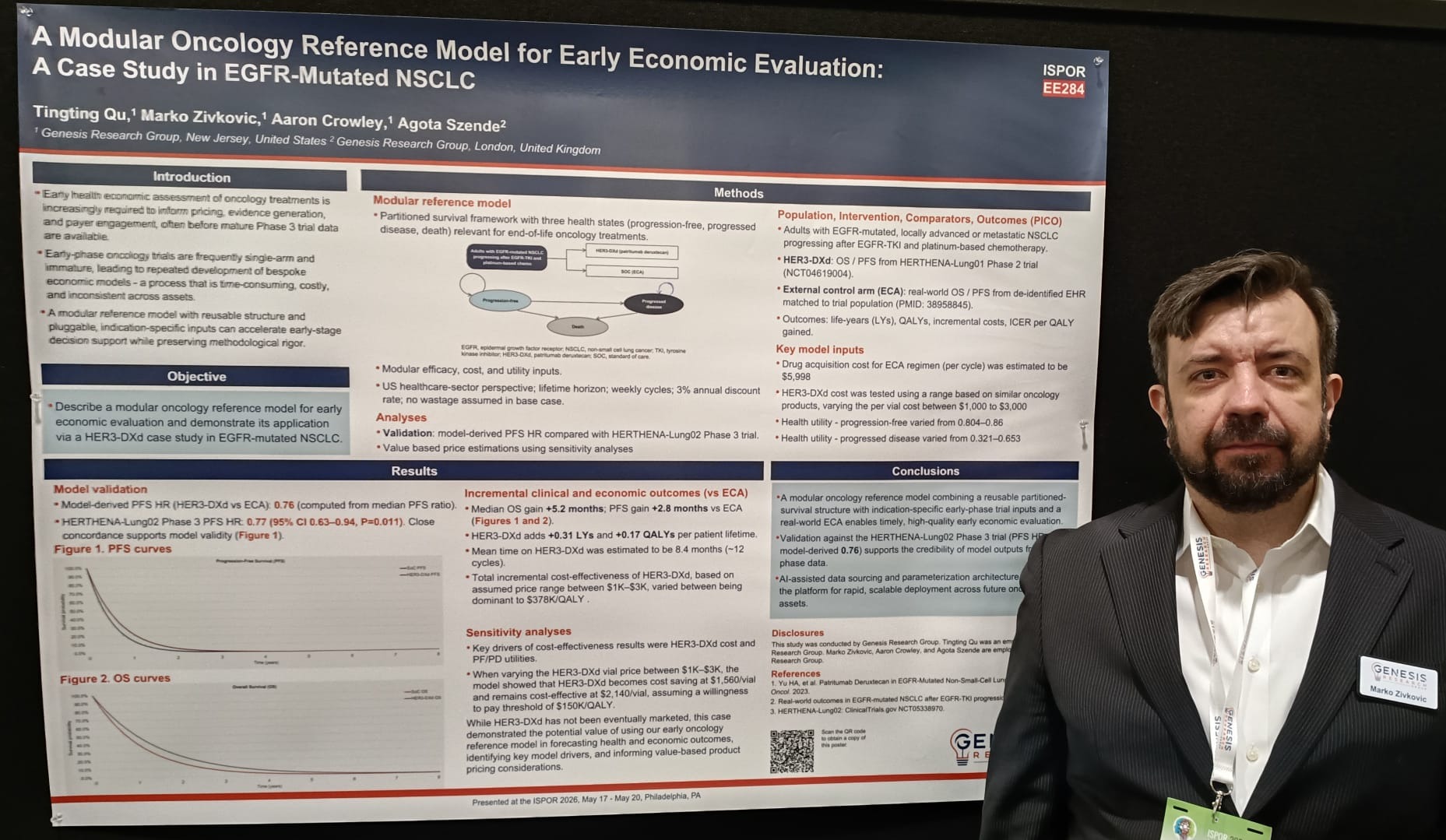
At ISPOR 2026, Marko Zivkovic, Head of Product, AI, Genesis Research Group, presented research describing a modular oncology reference model designed to support early economic evaluation in oncology, using a case study in EGFR-mutated non-small cell lung cancer (NSCLC).
In this interview, we speak with Marko's co-author, Agota Szende, Vice President and Head of HEOR Value & Evidence, Genesis Research Group, about the rationale behind the model, the methodological considerations involved in combining early-phase clinical trial data with real-world external controls, and the potential implications for early evidence generation, payer engagement, and future oncology decision-making.
Early economic evaluation is becoming increasingly important in oncology development. What challenges or evidence gaps prompted you to develop a modular reference model approach rather than relying on indication-specific economic models developed on a case-by-case basis?
Bespoke early models are time- and resource-intensive, and often require extensive future adaptation and reprogramming as data becomes available. The purpose of the reference model was to meet the needs of stakeholders to run analyses and ask key questions at an early stage where important decisions need to be made. Oncology models tend to follow a set partitioned survival framework, which models progression-free survival (PFS) and overall survival (OS) extrapolated beyond the timeframe of the clinical trials. Early models are typically based on the target product profile or single-arm trials. This creates a need for an external control arm (ECA) based on the natural history of the disease, which, in turn, allows for a more informative cost-effectiveness evaluation against standard of care comparators. The early model can also be rapidly parameterized as new data becomes available and can support the identification of key drivers in advance of developing the full cost-effectiveness model for global HTA submissions.
Could you outline how the modular oncology reference model was structured and how the ECA was incorporated into the analysis?
The presented oncology reference model is structured using a three-state partitioned survival model. The ECA was derived from a published real-world evidence (RWE) cohort of patients, which was digitized. The platform allows various parametric models to be fitted to extrapolate PFS and OS for the ECA. The treatment curves can either be developed by uploading the data into the platform or by applying a hazard ratio to the ECA.
What were the main methodological considerations or challenges when combining early-phase clinical trial data with a real-world ECA in this analysis?
In this example case, the model integrated an ECA analysis that estimated real-world OS/PFS from de-identified electronic health records (EHR) matched to trial population. Typically, the key challenges with such analyses are the inclusion of prognostic factors, dealing with clinical heterogeneity and small sample sizes, data quality, ensuring face validity and finding ways to minimize uncertainty overall around the comparative clinical assessment. A key approach in this case was to optimize the identification of a matched subset of patients by using propensity score (PS) weighting.
The PFS findings appeared broadly consistent with later Phase 3 results. How did you interpret those findings, and what did they suggest about the potential role of early modeling approaches?
The interesting finding that PFS and hazard ratios based on them used in the model were consistent with later phase results meant that the deterministic forecast for cost effectiveness from our early economic model was very accurate. However, it is important to note that there would be valid reasons why later phase study results would be different from those reported during early phases.
“As such, the role of early economic models should be interpreted as tools to test scenarios, identify key drivers, quantify ranges for maximum economically justifiable product price, and with that to inform strategic value-based pricing and market access considerations.”
Your analysis identified treatment costs and health utilities as major drivers of cost-effectiveness. Were there any findings or methods applied that are particularly relevant from a payer or HTA perspective?
It is not surprising that treatment costs, survival, and health utilities are key drivers in oncology health economic evaluation, particularly in the case of end-of-life treatments in indications where patients face a short life expectancy. From a payer and HTA perspective, however, it is essential that the model is transparent and validated and applies methods and data sources that are well established and relevant for their perspective, so as to minimize uncertainty and maximize the quality of their decision-making.
How do you see reusable or modular economic modeling approaches influencing evidence planning and payer engagement earlier in the oncology development pathway?
Oncology modeling typically involves extrapolation of trial data using complex methods to ensure a good model fit and clinical validity. The customization of the modular framework will allow the user to change the assumptions in a dynamic manner, which will facilitate discussions with payers. It will also allow payers to suggest their own assumptions and view the impact in real time.
“In early evidence planning, the reference model can also be used to inform study design for the later phases of the clinical trial program, such as endpoint selection, sample size estimation, response assessment, HEOR data collection alongside the trial, as well as informing payer focused analytic sections or supplements to the main analysis plan.”
Importantly, the early model can also be used to identify key data and evidence gaps and inform RWE data generation planning in a timely manner.
Looking ahead, how transferable is this modular framework across other tumor types or therapeutic areas, and what additional evidence or validation work would still be needed before broader implementation?
While initially we are validating the modular framework in oncology areas that are ideal candidates for the three-state partitioned survival approach, in the future we plan to expand the capabilities and validation of the model to capture a wider range of oncology areas. These include the use of mixture-cure models where the goal of treatment is to induce remission as well as landmark response-based models. Eventually, the application of alternative more complex model structures such as Markov cohort models and patient-level simulation will be validated and supported by AI agentic systems designed to support various aspects of the model and its further development.
About the interviewee
Agota Szende, PhD
Vice President, Head of HEOR Value, Genesis Research Group

Agota has 30 years of experience and specializes in the design and delivery of pharmacoeconomic models across all phases of product development, including health utility assessments, clinical trial-based HEOR research, and RWE generation. She has expertise in costing methodologies to support burden of illness and economic modeling studies, and the use of HEOR data in regulatory and reimbursement decision-making. As a member of the EuroQol Group, she has led task forces and published on self-reported health, preference valuation, and the application of the EQ-5D instrument in clinical and economic contexts. Agota has led multidisciplinary project teams supporting global life sciences clients with strategic health economic model development, country-specific adaptations, successful HTA submissions, and post-launch health economic tools and publications. Prior to joining Genesis, Agota served as a Health Economics & HTA Lead in the consulting field and has held health economist roles at MEDTAP International and AstraZeneca. She has authored over 70 publications and has published in top-tier HEOR and therapeutic area journals. She earned a PhD and MSc in Health Economics from the University of York.
Acknowledgments
The authors would like to acknowledge modeling and writing support from Alasdair Henry, Tingting Qu, Daniel Ribes, and Aaron Crowley.
Disclaimers
The opinions expressed in this feature are those of the author and do not necessarily reflect the views of The Evidence Base® or Becaris Publishing Ltd.

Sponsorship for this Interview was provided by Genesis Research Group.