Economic modeling in healthcare: harnessing stakeholder insights for real-world impact

In a dynamic healthcare landscape defined by evolving policies, shifting payer expectations, and changing pricing thresholds, stakeholder insights are essential to maintaining the relevance, adaptability, and effectiveness of economic models in addressing the needs of patients and healthcare systems. By integrating perspectives from clinicians, payers, providers, and patients into the development process, economic models are better positioned to withstand rigorous scrutiny in access and reimbursement evaluations, increasing their robustness and applicability in the real-world healthcare environment.
At ISPOR Europe 2024 (November 17–20, 2024, Barcelona, Spain), the presentation, "Planning with Insights: Even the Best Economic Models Need Validation," delved into this topic, exploring a roadmap for building robust, stakeholder-informed economic models that effectively support reimbursement decisions while addressing the complexities of global markets. Using a case study to illustrate the impact of insights on economic models, the session was led by Priti Jhingran (Genesis Research Group) and included contributions from Dominic Jones-Phillips (Genesis Research Group), Smita Kothari (Merck & Co., Inc.) and Carole Longson, MBE (consultant).
Economic modeling across drug development phases to inform decision-making
Priti Jhingran welcomed attendees to the session, which drew a capacity crowd.

The session began with an exploration of the role of economic models in supporting decision-making at various stages of drug development. In the early phases (Phase 1 and 2), modeling may include natural history models, disease characterization models, or early cost-effectiveness analyses to determine the minimum efficacy required for an asset to be both viable and cost-effective. As development progresses into late-stage clinical trials (Phase 3), cost-effectiveness models are used to better understand input parameters at both the disease and drug levels, allowing teams to identify knowledge gaps and address key issues where insights can make a substantial impact. Budget impact models are also employed to assess affordability of the asset in each market. Finally, in the post-launch phase (Phase 4), models may be needed for reassessment or to support product commercialization and differentiation, especially in a competitive environment.
Importance of stakeholder insights
“When you bake in insights in early stages of model development, you really have a higher likelihood of having a relevant model, as well as scientifically robust methodology used to develop the model. And what's most important is that you get the framework right for the model.”
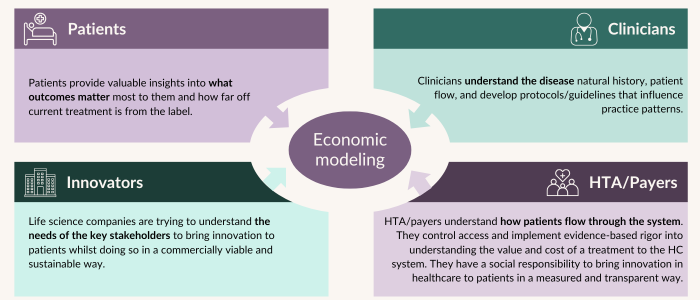
It was noted the framework of a model is akin to the foundation of a house; getting it right is essential for everything else to follow effectively. When developing the model, insights from different stakeholders bring different perspectives to inform key model components:
There are three key considerations for integrating insights into both the assessment framework and model development.
- Early engagement: Gathering insights early in both product development and model design is a critical step in creating robust, effective and actionable outcomes. Early engagement ensures that evidence generation is seamlessly integrated into the modeling process, supporting the achievement of desired objectives. This approach requires careful prioritization, particularly when addressing uncertainties that arise from the involvement of multiple stakeholders. While including all perspectives is ideal, practical constraints—such as time, resources, and decision-maker requirements—often necessitate trade-offs. Identifying what is most essential for the model and aligning these elements with stakeholder expectations helps create a framework that is both robust and purposeful.
- Clinical trial impact: Understanding clinical trial timelines and regulatory requirements is crucial. Early identification of factors like patient populations and outcomes helps avoid delays and ensures trials meet both regulatory needs and support appraisal packages for reimbursement.
- Evidence requirements: Generating real-world evidence (RWE) requires balancing feasibility with deadlines. Factors such as the availability of data, the infrastructure required for collection, and the expected time to generate meaningful insights must all be evaluated. Balancing these practicalities ensures that RWE contributes effectively to the model while remaining aligned with overall development goals.
Lastly, throughout model iteration, it is important to evaluate whether incorporating each insight will significantly reduce uncertainty for decision-makers. If not, certain insights may need to be deprioritized to focus on those that add the most value.
Patient insights are key
Patients are among the most critical stakeholders, and incorporating their input, along with that of their caregivers, is essential for achieving a comprehensive understanding of healthcare needs and outcomes. Their firsthand experiences provide invaluable insights into the disease, the care process, and the real-world impact of treatments. Engaging these voices helps uncover the lived realities of conditions, offering a foundation for models that accurately reflect real-world scenarios and support more informed and effective decision-making.
Patient experience data (PED) enhances economic models in health technology assessments (HTAs) by providing real-world insights into a product’s value. Metrics like quality of life (e.g., QALYs) and patient-reported outcomes (PROs) quantify the impact beyond clinical efficacy, addressing adherence, functionality, and ease of use. These data inform assumptions about indirect costs, subgroup variations, and societal benefits, tailoring models to reflect diverse needs. Additionally, patient insights support value-based arguments by highlighting unmet needs and projecting long-term outcomes where trial data is limited. Integrating PED ensures economic models are credible, comprehensive, and aligned with HTA expectations, strengthening the case for new products.
Globally, the integration of patient perspectives in HTA processes is expanding, emphasizing the increased focus on inclusivity and transparency. In the US, the Centers for Medicare and Medicaid Services (CMS) plans to enhance engagement with patients and advocacy organizations in the upcoming phase of drug pricing negotiations under the Inflation Reduction Act. Similarly, in Europe, the implementation of the new EU HTA regulation is strengthening patient involvement in HTA processes, ensuring that assessments account for the diverse experiences and needs of those directly impacted by healthcare decisions. In the UK, NICE includes patient and caregiver evidence in its appraisals to capture the lived experience of a disease and its treatment.
Understanding payer priorities
Moving to the payer insights, it was emphasized that the decision-maker is not an expert in modeling and does not delve into the detailed analysis of model inputs, parameters, or transition probabilities. What they want to understand is whether the model makes sense to them and resonates with the perspectives of their stakeholders, including clinicians and healthcare systems.
"It's a very different take, which is why all of the insights gathered early on, and all of the decisions, the choices you make a lot along the way, have a massive impact in the way that a non-technical decision-maker views that outcome."
The transition from assessment to appraisal amplifies the importance of a model's relevance. While some elements may be consistent across jurisdictions, it is crucial to validate the model structure for each specific context. If decision-makers perceive the model as flawed, they will scrutinize every detail. Therefore, being able to justify the chosen model structure and present the validation evidence becomes a critical narrative in the decision-making process beyond just technical considerations.
Considerable time and effort go into validating technical elements through stakeholder insights, enhancing the model's robustness. However, both robustness and relevance are equally important, with relevance being paramount for decision-makers. A model must first demonstrate its relevance before decision-makers will examine its robustness.
Payer insights are crucial, but payers serve as a proxy for broader stakeholders, including patients, clinicians, and policymakers. To develop a strong foundation for economic models, it is beneficial to engage directly with these individual stakeholders first and then cross-check, or ‘triangulate’ those insights with those provided by payers. This approach ensures a solid basis for creating models that are both robust and relevant, meeting the expectations of decision-makers effectively.
Importance of insights from the industry perspective
Economic models are vital in the industry's efforts to ensure products transition smoothly from development to the patients who require them. The process of economic modeling in healthcare decision-making can be approached from two aspects: 1) understanding the decision-maker; and 2) developing the model itself. These decision-makers—often payers or HTA bodies—use economic models to evaluate different aspects of a product before making decisions that could bring the product to patients. Understanding their criteria is essential for designing an effective model and so insight gathered needs to keep both of these aspects in mind.
The payer perspective often serves as the starting point for model development, but it is crucial to consider the diversity of decision-makers across different geographies. Not all countries have HTA processes, and among those that do, the frameworks may vary significantly. Decision-makers may include atypical stakeholders like wholesalers or private payers, whose needs must also be addressed. Additionally, collaboration and interdependence between decision-makers across regions can influence the model requirements, such as with immunization technical advisory groups in the vaccine space, which guide decisions that later impact payer actions.
From an industry standpoint, gathering insights when developing the model itself, there are two key components:
- The model framework (or the structural components)
- Input variables
The structural components, also called user non-modifiable components, are foundational, focusing on the natural history and progression of the disease, outcomes, and what impacts patients the most. These elements are typically country-agnostic and remain consistent throughout development. The work on these components begins early, even in Phase 1 or Phase 2 trials, to ensure that any necessary data can be gathered during the clinical trial process. Here, RWE can also be leveraged; for example, large natural history studies, which require a long lead time. This is an iterative process and insights from clinicians, patients, payers, policy makers and providers are included much earlier on.
Input variables, on the other hand, are more flexible and tailored to the specific market and stakeholder needs. Insights gathered at the right time ensures they remain current and relevant for decision-makers in each country. These user-modifiable variables may include epidemiology, treatment landscapes, and utilization rates, which can differ significantly across countries. RWE plays a key role, especially for markets with limited data. Insights from local decision-makers, patients, and providers help determine what evidence must be collected from each specific market versus what can be leveraged from other regions where early modeling work has already been conducted.
Case study: an insights-driven global cost-effectiveness framework for Duchenne muscular dystrophy (DMD)
To put this into context, the session included a case study on a cost-effectiveness model for Duchenne muscular dystrophy (DMD) to illustrate value assessment using incremental cost-effectiveness ratio (ICER). In DMD, the primary goal of treatment is to maintain patient mobility—keeping patients in the ambulatory stage. Maintaining ambulation is highly valued, as it leads to better clinical outcomes, minimal caregiver burden, and managed quality of life. The transition from ambulatory to non-ambulatory is significant, with increased healthcare costs, deteriorating quality of life, and a heightened caregiver burden. Therefore, any treatment that delays or prevents this transition is seen as a valuable asset for the DMD community.
To provide a life sciences company with stakeholder-centric insights into a cost-effectiveness model for a DMD treatment in early development, Genesis Research Group convened a HTA body/payer council. This council included payers, patient advocates, clinicians, and other key stakeholders involved in DMD research. The goal of the council was to address specific modeling challenges and identify gaps in the evidence package for DMD during the early stages of development.
One key insight gathered was the need to better understand the natural history of DMD. While the available natural history data was robust, it inaccurately suggested patients could live longer, contradicting established evidence of a shorter life expectancy. Early loss of ambulation significantly increases mortality risk. Addressing this discrepancy was crucial from the outset to ensure the model accurately reflected patient outcomes.
The case study underscored how stakeholder insights helped address specific modeling challenges; for example, existing natural history data for DMD was inconsistent with clinical observations due to insufficient mortality data. To mitigate this, the model was calibrated to better reflect real-world patient outcomes, and sensitivity analyses were conducted to explore alternative assumptions. These adjustments ensured that the economic model was more accurately aligned with the realities of DMD progression and treatment impact.
Additionally, as insights showed that as patients transition from ambulatory to non-ambulatory stages, their quality of life declines significantly, moving through multiple severe health states—from wheelchair use to becoming bedridden. However, the utility estimates lacked sufficient granularity to accurately reflect these changes. Based on the available data, it was evident that sensitivity analyses were needed to explore alternative assumptions for the natural history model and different data sources for DMD mortality estimates.
The final insight discussed related to the endpoints used in the Phase 3 program. Historically, the six-minute walk test had been the standard measure, but in this trial the North Star Ambulatory Assessment (NSAA) was used. However, many payers and clinicians were unfamiliar with this endpoint and this lack of awareness risked undermining the credibility of the evidence package when presented to an HTA body. These insights highlighted the importance of developing an effective communication strategy and generating additional evidence to establish the true prognostic value of the NSAA.
“What was really critical here was bringing multiple stakeholders together early on, allowing enough time to develop a mitigation plan and understand what adjustments were needed in the evidence package.”

Sponsorship for this Deep Dive was provided by Genesis Research Group. If you would like copies of the slides or have any questions, please contact [email protected].