Following the patient journey: How connected data and evolving methods are reshaping real-world evidence

During ISPOR 2026 Cardinal Health speakers examined the challenges of generating real-world evidence (RWE) from increasingly fragmented healthcare data. The discussion explored how first-party electronic health record (EHR) access, tokenization, physician-led data collection, and evolving analytical methods are helping researchers connect patient journeys and develop evidence suitable for clinical and regulatory decision-making.
The complexity of modern healthcare delivery presents a fundamental challenge for evidence generation. Patients with serious conditions such as cancer are rarely managed by a single clinician in a single setting; their care spans multiple providers, institutions, and data systems that are rarely fully integrated. Translating that fragmented clinical reality into research-grade evidence demands not only sophisticated data infrastructure, but also methodologies capable of capturing clinical detail at the granularity required for regulatory and decision-making purposes.
At ISPOR 2026, the session titled 'The Future of RWE: Claims and EMR Were Just the Beginning' explored precisely that challenge. Moderated by Amy Eaves (Vice President of Real-World Data and Evidence), the discussion brought together her colleagues Bruce Feinberg, DO (Chief Medical Officer), Harlen Hays, MPH (Senior Director of Scientific Operations and Analytics) and Andy Klink, PhD, MPH (Senior Director of Business Development, Real-World Data and Evidence). Drawing on Cardinal Health's evolving evidence generation programs, the session traced the limitations of conventional data sources, examined how data infrastructure has matured over the past decade, and outlined methodological innovations that have extended the scope of what RWE can support.
Understanding fragmentation across the patient journey
Opening the discussion, Eaves asked Feinberg how healthcare delivery has evolved and what researchers should understand when attempting to access health record data directly from treating physicians. Drawing on his experience as a practicing oncologist, Feinberg argued that many assumptions about healthcare remain rooted in an outdated model of a single physician caring for a single patient. In reality, modern care pathways often involve numerous providers operating across multiple settings.
Describing the typical trajectory of a lung cancer patient, he outlined involvement from primary care, pulmonology, thoracic surgery, medical oncology, radiation oncology, palliative care, and various imaging and pathology services, each potentially operating within separate data systems and organizational structures. As Feinberg observed;
"That complexity is something that is difficult to account for when we think simplistically about health information and evidence research."
This also extends beyond care delivery itself. Depending on the practice environment, clinically relevant information may be distributed across EHRs, hospital systems, imaging platforms, pathology systems, scanned documents, PDFs, and external specialist records. Even within a single organization, structured EHR data may capture only part of the patient story.
Feinberg noted that advances in precision medicine have further increased the challenge. Diseases once defined primarily by organ systems are increasingly classified according to molecular and genetic characteristics, creating smaller, more specialized patient populations and increasingly complex treatment pathways. At the same time, the volume of clinical research continues to expand, placing additional demands on evidence generation.
Generating research-ready evidence from fragmented data
Building on Feinberg's observations, Eaves asked what researchers must consider when attempting to generate data suitable for research within such a complex environment.
Hays explained that the challenge is not simply one of scale but of structure. While healthcare has undergone rapid digitization over the past two decades, the resulting data landscape remains fragmented.
Historically, many real-world studies relied heavily on administrative claims data. Although valuable for understanding healthcare utilization and billing activity, claims provide limited insight into the clinical circumstances surrounding treatment decisions. As EHR adoption expanded, researchers gained access to richer clinical information, but new challenges emerged regarding data consistency, completeness, and interpretation.
At the same time, important information remained outside structured datasets. Patient experiences, physician reasoning, disease characteristics, and treatment decisions were often documented within narrative clinical notes or not captured in standardized formats at all.
Hays emphasized the importance of working as close to the original clinical source as possible through first-party EHR access.
"By first party, we mean we're the first group to touch it," he explained, noting that this approach avoids potential information loss introduced through multiple layers of aggregation and transformation.
Direct access also creates opportunities to involve physicians in validating information and providing additional context. Rather than simply documenting what occurred, researchers can begin to understand why particular treatment decisions were made.
As Hays noted, this creates opportunities to capture information that extends beyond traditional structured data elements, including clinical reasoning and aspects of the patient experience that are often absent from conventional datasets.
Translating connected data into decision-grade evidence
Reflecting on the evolution of RWD infrastructure, Hays described a progression from relatively simple data warehouses toward increasingly connected evidence ecosystems.
Early efforts focused on extracting data from individual sources and storing them in centralized repositories. As researchers sought to incorporate physician notes, chart abstraction, specialty-specific datasets, and other sources, it became increasingly clear that no single database could adequately represent the complexity of modern healthcare.
This realization led to what Hays described as the "era of tokenization." As healthcare data became increasingly distributed across providers, systems, and care settings, the challenge shifted from collecting information to connecting it. He remarked:
"A siloed database is not enough. It doesn't give us the information we need. We actually need to connect the dots. We need to connect this person."
Tokenization enables researchers to link records across disparate sources while maintaining privacy protections, creating a more complete view of the patient journey and the care delivered along the way.
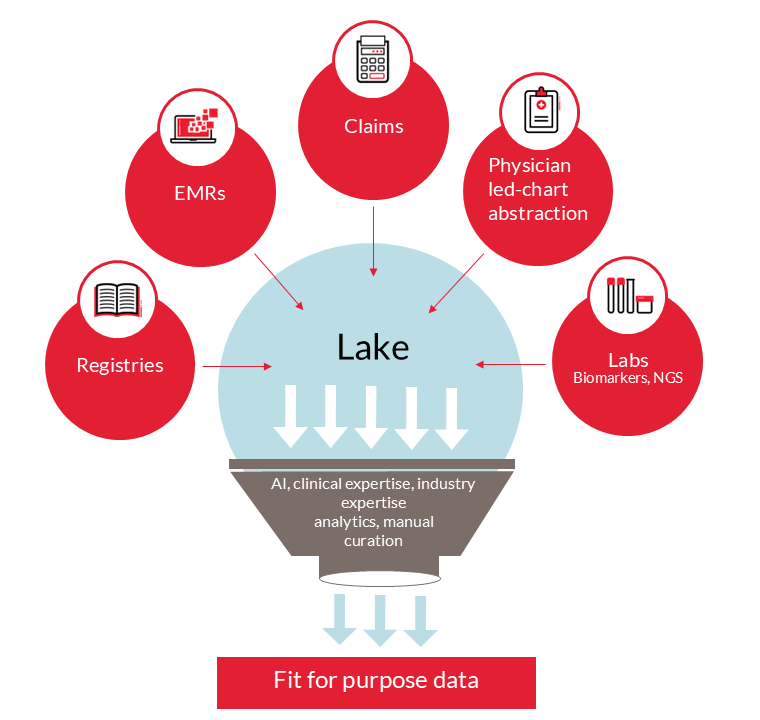
He described the emergence of data lakes, lakehouses, and other connected architectures designed to integrate information from diverse sources while preserving clinical context. The aim, Hays explained, is to create an environment that is "as close to the source of truth" as possible – one that is purpose-built for research while also having the potential to support physicians in understanding and acting on patient data.
These environments increasingly combine structured EHR data, unstructured clinical documentation, claims records, imaging data, pathology information, and physician-reported insights. Human curation remains an important component, but Hays also highlighted the growing role of AI-enabled approaches that can help extract information from unstructured sources and reduce the effort required to assemble research-ready datasets.
The goal, he suggested, is to spend less time compiling and building data assets and more time understanding what those data mean. But he cautioned that data alone are not enough. Researchers must also apply the right methodologies and ask the right questions if they are to transform connected data into meaningful evidence. The challenge, therefore, is not simply connecting the patient journey, but translating those connected data into reliable measures of treatment patterns, outcomes, and clinical benefit.
Developing endpoints that reflect clinical reality
Building on this theme, Klink examined how evolving methodologies are helping researchers generate evidence that more closely aligns with clinical research standards. Many of the limitations historically associated with RWE stemmed not from a lack of data, but from difficulties identifying appropriate patient populations and deriving clinically meaningful endpoints from routine care data. Early studies relying on claims or structured EHR data alone often struggled to capture the level of clinical detail required to answer questions traditionally addressed through clinical trials.
Physician-led chart abstraction emerged as one approach to addressing this challenge. Rather than relying solely on structured data, the approach enables treating physicians to abstract clinically relevant information directly from patient records, including laboratory reports, pathology records, imaging systems, and clinical notes. As Klink explained, the approach offered a unique opportunity to understand not only what treatment decisions were made, but also "the why, the reason behind treatment decisions." By incorporating clinical context and physician rationale, researchers were able to more accurately identify eligible patients, evaluate treatment patterns and outcomes, and better understand the factors influencing real-world clinical decision-making.
This foundation enabled the development of increasingly sophisticated real-world endpoints. Klink highlighted the development of real-world Response Evaluation Criteria in Solid Tumors (rwRECIST), which emerged from observations that assessments of treatment response in routine clinical practice often differed from those reported in clinical trials. Rather than relying solely on physician-reported responses, researchers applied established RECIST criteria to information contained within patient medical records, including lesion measurements derived from imaging reports. The goal was to generate response assessments that more closely mirrored those used in clinical trials while remaining grounded in routine clinical care.
Building on the rwRECIST framework and the ability to connect clinical, claims, and other RWD, researchers next turned their attention to hematologic malignancies through the development of real-world Lugano (rwLugano) methodologies. The work represented a further step in aligning real-world endpoints with clinical trial assessments and subsequently informed the development of an external control arm for a single-arm trial included in an FDA submission. According to Klink, the challenge was not simply identifying comparable patients, but ensuring both consistent endpoint measurement and sufficiently complete covariate data to enable robust matching between trial and real-world cohorts.
The example illustrated how advances in data connectivity and endpoint development are increasingly supporting regulatory applications. To further evaluate the robustness of these approaches, researchers compared rwLugano assessments with blinded independent central review (BICR), the gold standard for treatment response assessment in many oncology trials. Although obtaining and re-reading imaging scans is typically resource-intensive, the analyses found no statistically significant differences between rwLugano and BICR assessments, suggesting that carefully developed real-world methodologies may provide a practical alternative in certain research settings.
External control arms and the future of evidence generation
The discussion progressed to the broader role of external control arms in evidence generation. An audience member asked under what circumstances such approaches may be most appropriate.
Responding, Feinberg pointed to the continuing evolution of precision medicine and the emergence of therapies targeting increasingly rare patient populations. In some settings, patient recruitment may be exceptionally challenging. In others, therapies may demonstrate such substantial clinical benefit that prolonged randomized studies raise ethical concerns. He noted that the external control arm example emerged after slow recruitment threatened to significantly delay development timelines, prompting early engagement with the FDA to explore alternative approaches.
"There are 7000 single mutation hereditary diseases," Feinberg observed, arguing that the combination of highly targeted therapies and small patient populations is creating growing demand for new evidence-generation strategies.
From a data perspective, however, Hays cautioned that rarity alone is not sufficient. Researchers must still be able to identify enough patients within available data sources to construct meaningful comparator cohorts. The challenge is to identify patient populations for which conventional trial recruitment is difficult, while ensuring that enough patients can still be identified within available real-world datasets to support robust comparator cohorts. Importantly, he highlighted a fundamental distinction between clinical trials and RWD, saying:
"A clinical trial is sanitized, it's structured, it's exact, you have complete control over what data is going to be collected. RWD is the exact opposite."
As Hays explained, researchers must effectively create an "illusion of control," with matching methodologies playing a critical role in ensuring that real-world comparator cohorts are as comparable as possible to trial populations.
Klink noted that external control arms are also being considered in randomized controlled trials where comparator arms selected several years earlier may no longer represent the standard of care by the time the trial results become available. In rapidly evolving therapeutic areas, contemporary external control arms based on routine clinical practice may therefore provide more appropriate comparators than historical trial control arms.
Following patients across care settings
Looking ahead, Klink identified connectivity across care settings as one of the next major “frontiers” for evidence generation. Using bladder cancer as an example, he described how patients frequently move between urology and medical oncology settings as their disease progresses. While researchers may have detailed information from either specialty, understanding the complete patient journey requires the ability to follow patients across those transitions and connect care delivered in different settings.
Tokenization provides one mechanism for achieving this, enabling records generated across providers and specialties to be linked longitudinally. This allows researchers to move beyond isolated episodes of care and examine treatment pathways and outcomes across the full continuum of a patient's experience. The example reinforced a broader theme raised throughout the session: healthcare data fragmentation is not simply a technical challenge. It directly affects the ability to understand treatment decisions, evaluate outcomes, and generate evidence that reflects how care is actually delivered.
Defining fitness-for-purpose
In the final discussion, Eaves returned to a question that underpins many contemporary debates around RWE: how can researchers standardize disparate data sources and demonstrate that connected datasets are fit for purpose, particularly when evidence may be used to inform regulatory decision-making?
Responding, Hays argued that the answer lies less in achieving perfect standardization and more in understanding the relative strengths and limitations of different data sources. Rather than relying on a single definition, researchers should test whether findings remain consistent when alternative definitions are applied through sensitivity analyses. As he explained, the key question is: "As I change the data, did I actually see a change?" If the answer is no, confidence increases that the evidence is "directionally pointed toward the thing you're looking for.” For regulators and other decision-makers, transparency is equally important. Hays emphasized the need to clearly document how definitions were developed, how much customization was required, and whether others could reproduce the approach. Demonstrating that findings remain consistent under different assumptions helps establish confidence in the resulting evidence.
About the speakers
Amy Eaves
Vice President of Real-World Data and Evidence, Cardinal Health

Amy Eaves is a senior commercial leader with expertise in real world evidence, data strategy, and technology enabled consulting. As Vice President of Real-World Data and Evidence at Cardinal Health, she drives growth, strengthens client partnerships and advances data driven solutions that support life sciences innovation.
With more than 20 years of experience across healthcare, life sciences, and IT services, Amy has led high performing sales and delivery teams, scaled multimillion dollar portfolios, and consistently delivered double digit growth. Her career includes leadership roles at a large Clinical Research Organization and private equity backed technology services firms where she built new offerings, elevated customer success, and shaped go to market strategies in competitive, rapidly evolving markets.
Amy holds an MBA in International Business from Arizona State University and a BS in Molecular and Cellular Biology from the University of Arizona.
Bruce Feinberg, DO
Chief Medical Officer, Cardinal Health

Bruce Feinberg, DO, is Vice President, Clinical Affairs and Chief Medical Officer for Cardinal Health. He is nationally recognized for his expertise in specialty oncology and the business of specialty healthcare. Dr. Feinberg has been instrumental in the development of clinical pathways that aim to control costs, improve quality, and increase predictability, all of which are key factors in developing a sustainable approach for caring for patients with high-cost diseases.
Dr. Feinberg maintains his license as a board-certified medical oncologist in the state of Georgia where he practiced for 23 years after completing his fellowship at M.D Anderson Cancer Center. A highly sought-after researcher and speaker on healthcare policy, value-based care, and real-world evidence research, Dr. Feinberg is the author of the bestselling Breast Cancer Answers and its follow-up book, Colon Cancer Answers. He has been consulted by prominent national media outlets, including the New York Times, Wall Street Journal, Forbes, and CNN. Dr. Feinberg is Host of The Weekly Check-Up on WSB Radio in Atlanta and The Weekly Check-up Podcast. With The Weekly Check-Up, he provides the community with the latest health information and an opportunity to express their views on health and medicine.
Harlen Hays, MPH
Senior Director of Scientific Operations and Analytics, Cardinal Health

Harlen D. Hays, MPH serves as the Senior Director of Scientific Operations and Analytics. He directs a team of senior scientists, statisticians and data scientists in the conduct of statistical analysis and database management of real-world data from medical chart reviews, administrative claims databases, electronic medical record databases, and other sources for biopharmaceutical manufacturers seeking to generate real-world evidence for internal and payer projects, medical communications, and regulatory bodies.
With over a decade spent at the Cerner Corporation leading research, analytics, and data science projects for multiple markets, he also served as the Principal Investigator for the HIV Outpatient Survey (HOPS); a grant funded by the Centers for Disease Control and Prevention. Mr. Hays also has experience working as an Epidemiologist for the State of Kansas with a focus in Substance Abuse prevention, has a Bachelor of Science in Microbiology and a Master’s in Public Health from the University of Michigan.
Andy Klink, PhD, MPH
Senior Director of Business Development, Real-World Data and Evidence, Cardinal Health

Andy Klink oversees a team of Business Development Directors who support clients in conducting studies involving real-world evidence, pharmaco-epidemiology, health economics, and outcomes research in a range of therapeutic areas with a focus in oncology, rheumatology, urology, and gastroenterology. He has over 15 years of experience in academia and industry with health economics and outcomes research, multi-level mixed-effects analysis, longitudinal analysis, comparative effectiveness, and patient-oriented research. Serving as strategic scientific oversight and business development, Klink currently supports the development of industry-sponsored research studies involving administrative claims data, electronic health records, chart reviews, and patient and physician surveys to assess healthcare resource utilization, costs, quality of life, treatment patterns, treatment response, and other clinical and patient-centered outcomes. More broadly, Andy provides strategic real-world evidence for biopharmaceutical manufacturers to communicate value messaging to various healthcare stakeholders including regulatory agencies, payers, providers and patients.
Disclaimers
All opinions expressed are those of the speakers and do not necessarily reflect the views of The Evidence Base® or Becaris Publishing Ltd.
![]()
Sponsorship for this Deep Dive was provided by Cardinal Health.