Deep Dive: Understanding payer perceptions of health inequalities in health technology assessment and reimbursement decision-making
Disparities in health outcomes and access to health care among different population groups are becoming increasingly important to be considered in health technology assessment (HTA) and reimbursement decision-making. To ensure that health inequalities are appropriately and systematically considered by all stakeholders, there is a need for a clear framework, better methods to measure inequality, and a shared understanding of how these factors should be considered alongside clinical outcomes.
In the ISPOR 2024 session titled, "Payer Perceptions of Health Inequalities in Reimbursement Decision Making: Implications for the Pharmaceutical Industry," Kuldeep Singh and Tijana Ignjatovic of Genesis Research Group delved into this complex landscape. They shared results from a qualitative payer survey on perceptions of health equity and its role in decision-making, providing valuable insights into current stakeholder views on this critical issue.
Health inequity in HTA and reimbursement decision-making: current perspectives
Kuldeep Singh set the scene by referencing the WHO and NICE definitions of health inequity, highlighting a shared description of the term as, “an unjust, avoidable, and systematic difference in health outcomes and access to health resources among different population groups.” Looking at the available literature, Singh revealed that while some HTA agencies consider health equity in their decision-making, published frameworks are sparse. Notably, agencies like NICE and ICER have guidelines, but others, like HAS in France, do not. Even with existing frameworks, health inequalities are not consistently incorporated into HTA decisions. Various methods, including distributional cost-effectiveness analysis and multiple criteria decision analysis, can address health equity, but these approaches are still in their early stages and have their own complexities. Therefore, it is crucial to monitor how HTA methods and requirements will evolve.
To explore this further, Kuldeep Singh introduced Tijana Ignjatovic to share results from a survey conducted by Genesis Research Group on stakeholder views of health inequalities and their impact on the pharmaceutical industry.
Payer survey: measuring current payer perceptions of health inequalities and implications for the pharmaceutical industry
The survey included 31 current or former payers and representatives from health technology organizations across six key markets, chosen for their geographic diversity and representation of various payer system archetypes. Respondents held diverse roles, ensuring a range of perspectives and priorities.
In the US, participants included managed care organization payers, integrated delivery network payers, and population health managers. Brazilian respondents represented both public and private payers, while French participants included former transparency commission members and pricing committee members from the Comité Economique des Produits de Santé (CEPS). Italian and UK respondents provided both national and regional payer perspectives, and China was represented by national payers.
The survey was conducted via the Rapid Payer Response (RPR™) platform from Genesis Research Group – an online tool designed for quick, robust, and dynamic engagement with stakeholders. This agile platform allows for fast turnaround times, sometimes as short as 5 days, and facilitates ongoing feedback through follow-up questions. It leverages an extensive, pre-recruited, and pre-vetted network of stakeholders, ensuring that the most relevant respondents are selected to provide insights for each specific project.
What do stakeholders perceive to be the key drivers of health inequalities?
Tijana Ignjatovic went on to discuss the survey results. The 31 survey respondents were asked to allocate points out of 100 to potential drivers of inequalities. The pooled data showed:
- Socioeconomic status: Identified as the primary driver, encompassing factors like access to care, income, education, and living conditions.
- Race or ethnicity: Ranked second and notably flagged in the US, UK and Brazil – countries with higher proportion of different ethnic minority groups. Race and ethnicity have a strong correlation to socioeconomic status and are often influenced by systemic biases and lack of understanding of healthcare needs.
- Age: Generally seen as less relevant, although stakeholders in the US, UK and China highlighted access challenges for the elderly, such as lower Medicare reimbursement rates in the US and potential ageism in resource allocation.
- Gender: Highlighted in the UK and US due to differences in symptomatology recognition and lack of prioritization of women's health conditions.
- Genetic disposition: Viewed as a minor factor, as it is largely unavoidable.
- Regional disparities: Noted by stakeholders in Italy and Brazil, driven by economic development differences in Italy (North vs South) and infrastructure challenges in remote areas of Brazil.
Which specific factors should be prioritized from the payer's standpoint to mitigate health inequality?
To address this question, survey stakeholders were asked to review a set of potential factors, select the top five and rank them in order of priority.
- Access to care: Emerged as the foremost priority due to its deep-rooted connection to societal and contextual factors such as income, government support, and capacity to pay. This issue is perceived as unjust and modifiable, falling within the payers’ sphere of influence.
- Wider determinants of health: Ranked second by the survey respondents, these determinants heavily correlate with socioeconomic factors like education, housing, and employment status, influencing overall health outcomes.
- Ethnicity: The third most relevant factor, considered modifiable as it can be influenced by cultural and economic factors in addition to genetics.
- Differences in risks due to behavioral factors: A more partially modifiable factor influenced by cultural, regional, and ethnic differences.
- Biological factors: Differences in outcomes due to biological factors, such as treatment response, was generally viewed as not controllable.
- Quality and experience of care: Considered less relevant than access to care, especially within public health systems.
Which patient populations do stakeholders consider most important as meaningful targets for reducing health inequalities?
To understand these views, stakeholders were asked to rate the meaningfulness of health inequality reduction to different patient populations on a scale of 1 to 5, as shown in the figure below.
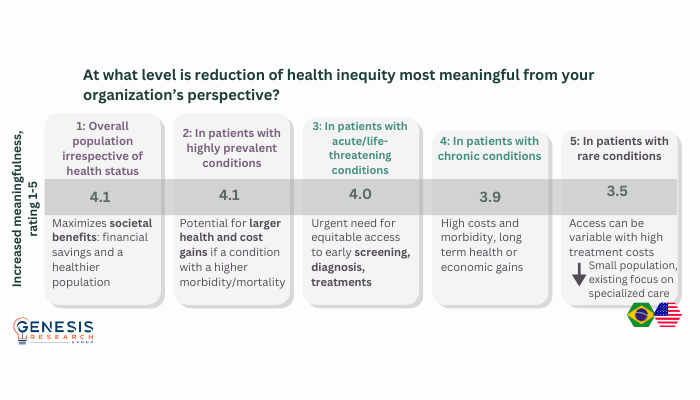
Ignjatovic highlighted patients with rare conditions, noting divided opinions among stakeholders. Some express concerns about high costs and lack of uniform access to treatment, particularly for orphan drugs; however, others, primarily in the US and Brazil, perceive access for these patients as relatively open, or prioritized through special government programs. Specific conditions mentioned for health inequality reduction focus include diabetes, obesity, mental health, women's health, and communicable diseases like HIV. The need to ensure high vaccination rates across all ethnic groups and populations with lower socioeconomic status has also been a topic of discussion among stakeholders.
How do stakeholders expect HTA agencies to evolve when considering health inequalities in decision-making?
Stakeholders were asked if they expect the importance of assessing the impact of a pharmaceutical intervention on health inequalities in the future to increase, decrease or stay the same. Across the board, respondents unanimously anticipated its increased significance, aligned with goals of optimizing health and economic outcomes for the population. Ignjatovic noted that meeting this expectation necessitates several evolutions within HTA and payer systems, with the need to:
- Formalize health inequality considerations in the HTA process across the board and apply consistently
- Contextualize inequalities within the disease burden – understand the populations that are affected and to what degree
- Subgroup analysis by different groups, such as race, age and ethnic groups, to understand how marginalized or underserved populations are affected
- Implement advanced methods such as DCEA
Most stakeholders also identified several barriers to this being implemented. Data availability poses a primary challenge, particularly concerning subgroup analysis related to socioeconomic status. Additionally, translating benefits into tangible health equity gains and cost savings proves difficult. Changes in HTA frameworks are necessary but complex and time consuming, particularly due to limited experience and lack of familiarity with many advanced methodologies. Cultural inertia also presents a risk, particularly with payers and HTA agencies balancing potentially conflicting priorities around economic pressures and improving equity. Despite these challenges, stakeholders agree that considering health inequalities will become increasingly important.
What are the most important initiatives for pharmaceutical manufacturers in achieving this goal?
The survey respondents were asked to rate (on a scale of 1 to 5) a series of potential activities that pharmaceutical manufacturers could undertake to advance health equity. The results are shown in the figure below.
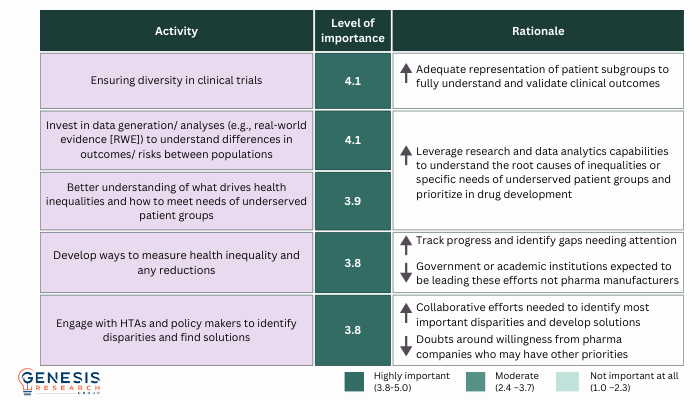
Ignjatovic noted that diversity in clinical trials has long been a priority for many organizations aiming to enhance the generalizability of trial results and ensure adequate representation of various racial, ethnic, and socioeconomic groups that mirror real-life demographics. She also called on pharmaceutical manufacturers to support data generation and analysis.
“This is where the industry can really help by leveraging research and data analytics capabilities to be able to understand the root causes of inequalities, to characterize them within relevant populations, and to understand what specific needs of the underserved groups need to be addressed. And then to include them in the clinical trial programs for drug development.” Tijana Ignjatovic, Genesis Research Group, ISPOR 2024
What are the least important initiatives for pharmaceutical manufacturers in achieving this goal?
Ignjatovic provided further insights from the survey, explaining that stakeholders also view certain activities as less relevant for pharmaceutical companies within the goal of improving health equity. These activities are often perceived to fall within the purview of health system providers or governments. For instance, initiatives such as partnering with payers, HTAs or providers to enhance patient journeys and diagnostic infrastructure are deemed valuable but challenging, with some stakeholders deeming they are better suited for government or provider intervention. Similarly, while patient support programs and education programs can aid disease awareness, disease management and empowerment, their effectiveness varies across regions. Stakeholders from the US, for instance, highlighted the need for these existing systems to be more precisely targeted from an inequalities perspective. In France, there is a sense of potential risk associated with undue influence whilst stakeholders in China expressed concerns about feasibility challenges due to the vast geographic expanse of the country. Lastly, the importance of HCP education regarding inequalities was acknowledged, but it was seen as primarily the responsibility of medical societies and governmental organizations.
What are the key takeaways for pharmaceutical manufacturers?
Ignjatovic provided three key considerations for pharmaceutical manufacturers based on the results of the survey.
- Identify socioeconomically impacted conditions and prioritize their development to address resulting inequalities.
- Provide and make data available to measure and address inequalities for both payer and HTA decision-making.
- Ensure diversity in clinical trials, invest in understanding health inequalities in key diseases, and share this information with payers and health system providers.
If you would like to find out more about RPR and the accelerated stakeholder insights provided by Genesis Research Group, visit their website or contact [email protected].
About the speakers

Tijana Ignjatovic, Executive Director, Genesis Research Group, UK
Tijana Ignjatovic is an Executive Director within the Access and Pricing Team and has over 15-years of consultancy experience in market access. In her time both in analysis and consultancy roles, Tijana has worked on multiple research methodologies and applied this experience, along with her market access knowledge, to lead and deliver numerous payer research projects in a broad range of therapeutic areas, including oncology, cardiovascular, infectious diseases, neurology, rheumatology, and many others. With a keen eye for detail, Tijana leverages her deep understanding of the industry and market access to quickly visualize and make connections on complex projects and provide strategic input to optimize clients’ market access strategy and value messaging across different payer requirements.

Kuldeep Singh, Executive Vice President, Genesis Research Group, UK
Dr Kuldeep Singh is a physician and healthcare expert with 20+ years of industry experience. He specializes in HTA, market access, HEOR, RWE, and pricing for pharmaceuticals and vaccines. He held senior positions at Novartis and WHO, and has executed diverse projects in market access, pricing, health economics, and HTA for companies across Europe and USA. He has an MPH from University College London/Humboldt-Universität zu Berlin/Karolinska Institutet, and an MBA from London Business School.
Sponsorship for this Deep Dive was provided by Genesis Research Group