Connecting real-world datasets to provide deeper insights into the patient journey

At ISPOR Europe 2025, Bruce Feinberg and Nicholas Lazarou of Cardinal Health assessed practical methods for improving real-world evidence through connected datasets. Their session explored data-integration challenges, the contribution of community networks, and how platforms such as SoNaR can enhance survival analyses and support more robust, regulatory-grade evidence.
Long-term outcomes are difficult to assess using real-world evidence (RWE), particularly when community-practice data are incomplete, inconsistent, or fragmented across systems. Improving data capture in these settings is essential to bridge the persistent gap between clinical trials and real-world experience. Doing so requires moving beyond structured fields and curating information from multiple sources to build a complete view of each patient’s treatment journey.
At ISPOR Europe 2025, the session “The Real-World Mosaic: Uniting Data to Illuminate the Patient Experience” examined these issues through the lens of Cardinal Health’s experience in urology and oncology. Moderated by Bruce Feinberg (Chief Medical Officer, Cardinal Health) and featuring Nicholas Lazarou (Sr Director, Clinical and Scientific Insights, RWD/E, Cardinal Health), the discussion focused on practical methods for integrating heterogeneous real-world data (RWD) sources into a coherent analytic structure. The session assessed technical, operational, and methodological considerations involved in creating a “real-world mosaic” of evidence. This Deep Dive explores the session’s key themes.
Why traditional trial evidence falls short in real-world settings
Feinberg began by examining foundational limitations of randomized controlled trials (RCTs). He noted that although RCTs remain the standard for regulatory decision-making, their design introduces constraints that limit their utility for understanding real-world outcomes. The cost and duration of trials delay the translation of innovation from research to practice, and their strict inclusion criteria often exclude patients with comorbidities, lower health literacy, or socioeconomic barriers. This creates evidence that does not fully represent the populations who later receive the therapy in routine care.
Feinberg emphasized that while the US system is unique in the degree of its fragmentation, similar structural and interoperability challenges affect healthcare systems globally. He explained that the US lacks a unified national health system, which results in “systems [that] don’t talk to each other” and incomplete data capture across settings. Despite these differences, he noted that many countries experience divergence between technology adoption, clinical workflows, and standardization, creating analogous barriers to complete evidence generation.
Barriers to building complete and connected real-world datasets
Lazarou outlined the central barriers to achieving integrated RWE, identifying three recurring challenges:
- Patient attrition
- Data fragmentation
- Inconsistent coding
He explained that patients “move, change providers, or stop engaging,” which interrupts the continuity required for longitudinal analysis. Fragmentation arises because RWD sits across multiple environments, including electronic medical records (EMRs), claims, registries, laboratory systems, and patient- and clinician-reported tools. Each contributes valuable information but does so using different formats, taxonomies, and levels of clinical precision. As Lazarou noted, these differences “give us integrative challenges within the data ecosystem.”
He stressed the need for standardization through “a common, standardized ontology” to support harmonization at the analytic stage. The aim is to identify the core dataset and supplement it with information that is “additive, not duplicative,” ensuring that the analytic environment is enriched rather than distorted by heterogeneity.
Feinberg then expanded on the “inherent complexity” of individual data sources. Electronic health records contain structured fields, unstructured notes, and clinically relevant details that may never be charted. Claims data are fully structured but lack clinical nuance. Additional material sits in PDFs, hospital records, and documents created by external specialists. According to Feinberg, “this lack of interoperability and this complexity just within one sphere adds to that complexity that has to be solved in putting all those pieces of a puzzle together.”
Returning to the broader integration challenge, Lazarou encouraged the audience to “think of it more as a mosaic.” Each data source represents a tile that offers only a partial view until combined with others. He noted that structured data alone cannot capture adherence, quality of life, or social determinants of health, which require careful curation. He also highlighted that 85% of care is delivered in community settings, meaning patients move between academic centers, hospitals, urgent care, and specialty pharmacies. This makes it essential to “distill it down to the belly button receiving the care,” ensuring all information is linked at the patient level.
Community networks as the foundation for integrated evidence
Feinberg transitioned the discussion to the infrastructure necessary to support data integration. He explained that understanding the patient journey requires more than aggregating data sources. It also requires close engagement with the clinical providers who generate those data. In his words, “the treating physician becomes a critical element” in ensuring that evidence reflects the realities of care rather than the abstractions of datasets.
Lazarou expanded on the infrastructure underpinning Cardinal Health’s RWD and RWE activities by outlining the role of group purchasing organizations (GPOs) in community practice. He explained that GPOs support clinical and economic efficiency by negotiating contracts, improving access to therapies, and reducing overall costs for practices. These networks also supply a critical layer of RWD that helps fill the “white space” often present in electronic medical records. According to Lazarou, the GPO structure provides a foundation for Cardinal Health’s evidence generation activities while also delivering value back to practices by reducing attrition, increasing diagnosis rates, and strengthening treatment consistency. He described this as “assuring that patients are navigated to the right care at the right time,” which he noted is central to improving outcomes across community settings.
Across these networks, more than 7000 providers are represented, including approximately 4000 urology providers operating across 730 private practices and more than 150 in-office dispensaries. This creates a vertically integrated community setting that captures prescribing, dispensing, diagnostics, and follow-up care across the same ecosystem. The in-office dispensaries are particularly important because they allow therapies that would normally require specialty pharmacy fulfillment to be administered on site. This improves adherence, reduces delays in treatment initiation, and provides more complete RWD on real-world utilization.
Feinberg noted that these structures effectively create an integrated ecosystem within the fragmented national context of the US. Although not equivalent to a unified national health system, they allow for a more continuous and traceable patient journey, which is essential for long-term outcomes analysis. He emphasized that “you need a technology platform that is going to integrate all the data, not just integrate the professionals who are the resource for that data.,” explaining that such integration also creates value that can support evolving research needs.
Tokenization and multisource integration via the SoNaR platform
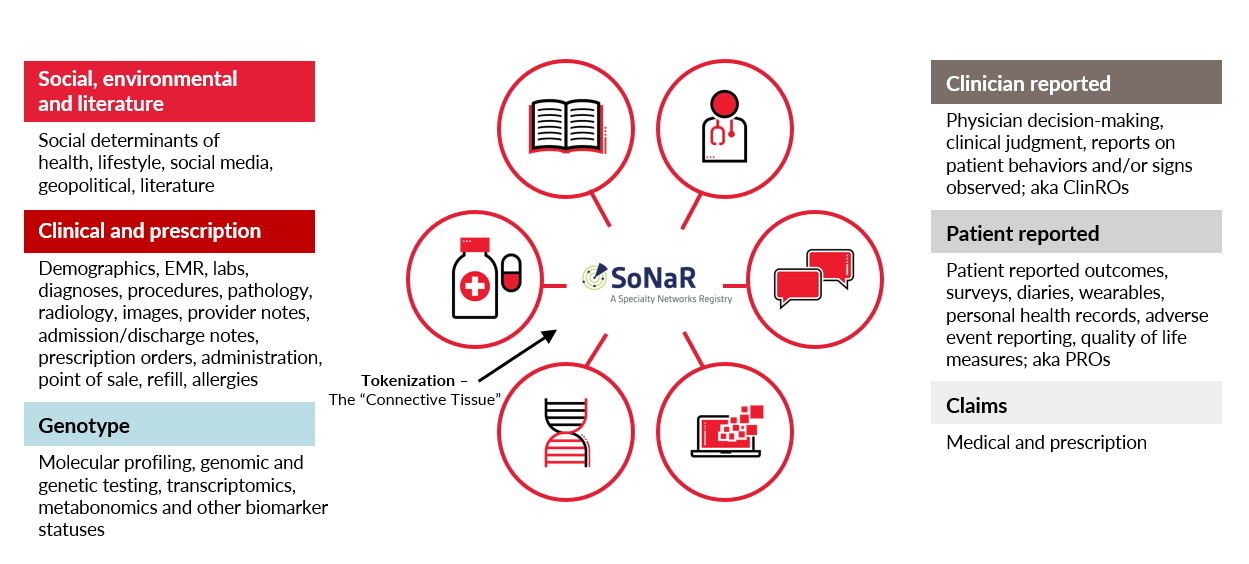
The discussion then shifted to Cardinal Health’s technical approach to data integration through SoNaR, the core platform supporting its RWD and RWE activities. Launched in 2022 in urology, SoNaR tokenizes data across more than 35 EMR and practice-management systems and other HIPAA-compliant, regulatory-grade sources. Lazarou explained that the community-based EMR is the focal point, with tokenization enabling linkage to preferred claims providers and achieving “over a 96% overlap of all of our patients” within the urology ecosystem. He noted that this approach “reduced a lot of white space” by capturing referral patterns, care received across settings, and other critical information that would not appear in an EMR-only dataset. Their oncology instance of SoNaR is scheduled for release in 2026.
The platform harmonizes clinical, claims, laboratory, next-generation sequencing, clinician-reported outcomes, and patient-reported outcomes, creating a unified, physician-centric analytic ecosystem capable of reconstructing a more complete treatment journey. Lazarou noted that this structure enables researchers to evaluate referral patterns, treatment sequences, genomic profiles, and clinical decision pathways within a single framework. He emphasized that incorporating somatic and germline testing is essential in uro-oncology, and that integrating clinician- and patient-reported outcomes is equally important for capturing both therapeutic effects and “the reasons why a clinician may make a decision.”
Case study: Evaluating long-term survival outcomes in community settings
Lazarou presented a case study illustrating the impact of connected community data. He described Cardinal Health’s long-standing relationship with Dendreon, the manufacturer of the personalized immunotherapy Provenge, indicated for metastatic castration-resistant prostate cancer (mCRPC). Beginning in 2014, the urology GPO partnered with Dendreon to support access, implementation, and provider education related to the therapy.
Using the integrated data environment established through SoNaR and the urology GPO, Cardinal Health conducted a long-term RWD study evaluating 5-year overall survival for Provenge in men with mCRPC drawn from 90 US community urology practices with over 3200 providers. The analysis identified an ~43months of survival among Provenge-treated patients.
Feinberg contextualized the findings by recalling the initial hesitation among physicians when Provenge was first introduced. The therapy produced what he described as a “profound tail to the curve of survival,” a pattern that was unfamiliar to many clinicians at the time. Its reliance on patient-specific cell manufacturing created logistical challenges and workflows that differed from conventional oncology treatments. Feinberg explained that once community practices had the necessary infrastructure, training, and integrated data systems in place, utilization increased and the long-term survival benefits became more evident.
The case study illustrated how integrated evidence environments can reveal treatment effects that were not apparent in earlier trial data. It also demonstrated how the mosaic model can support evaluation of therapies with complex administration pathways or long-duration survival patterns.
Use case: Supporting clinical trials through tokenized data and integrated networks
Building on the Provenge case study, the speakers then turned to the broader implications of connected datasets for clinical research. Lazarou explained that tokenization and integrated EMR data enable precise patient identification for trial recruitment. He noted that Cardinal Health works closely with CROs that face enrolment challenges, providing access to research sites within their networks and using SoNaR to match inclusion and exclusion criteria “with precision” at the site level. This approach has delivered meaningful time-to-value gains for CROs seeking eligible participants. He added that tokenized datasets also support physician-led chart abstraction and large-scale data integrations that enhance outcomes analysis for trial-related use cases.
Feinberg described a complementary application: the development of external control arms. He explained that real-world datasets can be used to construct regulatory-grade comparators, particularly valuable in oncology where rare molecular subtypes make traditional Phase 2 or 3 studies difficult to complete. By matching trial participants to real-world patients through multivariate criteria, external control arms can be built in 1–2 years rather than the 5–6 years often required for conventional trials. Feinberg noted that this approach enables them to “work in concert with clinical trials,” providing longitudinal follow-up while helping shorten the time to trial success.
Broader considerations for RWE generation
Lazarou concluded by outlining key priorities for strengthening RWD and RWE. He emphasized that high-quality evidence begins with consistent and comprehensive data capture in community-practice settings, noting that “the better the information on the way into the EMR, the better the information on the way into the database.” Improving the integration of patient-reported and clinician-reported outcomes remains essential for understanding treatment rationale, symptom burden, and quality-of-life impacts. Lazarou also highlighted the need for greater standardization to support regulatory-grade evidence and enable more efficient generation of RWE in routine practice.
Feinberg concluded by reinforcing the central role of clinicians in advancing RWE. He emphasized that engagement “is more than just collecting their data” and requires programmatic involvement that supports clinical workflow, meets professional needs, and demonstrates value to practice operations. Such engagement produces RWD that is more complete, reliable, and relevant, enabling evidence that is fit-for-purpose across industry, policy, and public health. He closed with a clear message about the broader ambition for the field:
“RWE must reach a level where it not only answers questions for industry, but also answers questions for society, and helps accelerate innovation by reducing the time it takes to bring new therapies to market.”
About the speakers
Bruce Feinberg, DO
Chief Medical Officer, Cardinal Health

Bruce Feinberg, DO, is Vice President, Clinical Affairs and Chief Medical Officer for Cardinal Health. He is nationally recognized for his expertise in specialty oncology and the business of specialty healthcare. Dr Feinberg has been instrumental in the development of clinical pathways that aim to control costs, improve quality, and increase predictability, all of which are key factors in developing a sustainable approach for caring for patients with high-cost diseases. A highly sought-after researcher and speaker on healthcare policy, value-based care and RWE research, Dr Feinberg has over 200 publications in peer-review; and he is also the author of the bestselling Breast Cancer Answers and its follow-up book, Colon Cancer Answers.
Nicholas Lazarou, MPH, MBA
Sr Director, Clinical and Scientific Insights, RWD/E, Cardinal Health

Nicholas Lazarou, MPH, MBA, is an accomplished epidemiologist and expert methodologist driving innovation in health informatics and pharmaceutical analytics. As Sr Director of Clinical & Scientific Insights at Cardinal Health, he leads strategies that advance RWE and specialty care. Products under Nick’s leadership include intelligence visualization and delivery programs that optimize standards of care, clinical research, business operations, and payor contracting. His leadership helped propel Specialty Networks’ successful acquisition and continues to shape data-driven solutions impacting thousands of providers nationwide. A frequent contributor to peer-reviewed research and industry panels, Nick champions rigorous methodology to improve outcomes and deliver measurable value.
![]()
Sponsorship for this Deep Dive was provided by Cardinal Health.