Beyond access: how wealth and race shape GLP-1 treatment outcomes in diabetes and weight loss

At Forian, we believe that analyzing patient cohorts aligned not only with general healthcare trends but also with how treatments are represented in popular culture is important. This approach helps gauge public perceptions and misconceptions, ensuring that scientific advancements are communicated effectively and can be embraced or critically assessed by the broader community.
In this Guest Column, Mike Sicilia, RWE Data Scientist, Forian, describes how data analytics capabilities have uncovered significant patterns in the accessibility and effectiveness of Glucagon-like peptide-1 (GLP-1) therapies, shedding light on how socioeconomic factors such as race and wealth impact patient outcomes.
Real-world data indicates socioeconomic disparities in GLP-1 therapy
GLP-1 receptor agonists, commonly used to treat type 2 diabetes (T2D), have become a popular weight-loss option. At Forian, a life sciences company combining cutting-edge healthcare data analytics with real-world insights, we conducted a study utilizing CHRONOS – a hybrid data ecosystem that includes insurance claims data and electronic health records (EHR). The study revealed deeper narratives behind GLP-1 treatment access and outcomes. As GLP-1 therapies continue to be utilized for both diabetes management and weight loss, these findings can highlight the importance of socioeconomic factors in patient outcomes and healthcare accessibility.
After analyzing our data ecosystem, 134,000 patients were identified from 2015 to 2023, based on the study criteria of at least one baseline BMI reading (within 30 days before GLP-1 initiation) and at least one follow-up BMI reading some time after initiation. This allowed for measuring longitudinal differences in BMI across the study population and segmentation of the differences by both race and net worth, two key socioeconomic status indicators. These patients were classified as either non-diabetic or diabetic and studied separately. Non-diabetic patients were studied for how wealth and race affected GLP-1 initiation and BMI variations. Diabetic patients were analyzed for patient out-of-pocket impact.
Beyond diabetes: how wealth and race influence GLP-1 usage
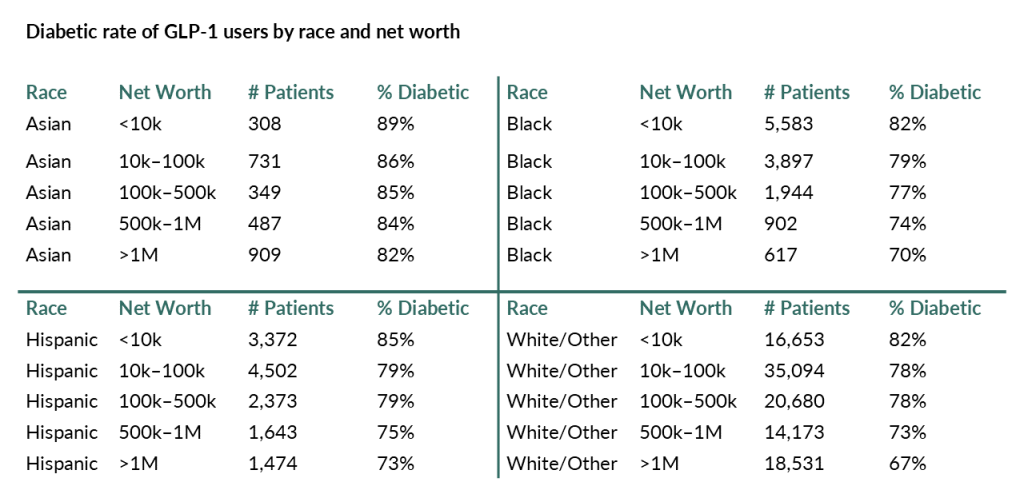
GLP-1 medications are often associated with treating T2D, but recently their reach has started to extend beyond just diabetic patients. To understand broader usage of GLP-1s, this analysis of non-diabetic patients focused on the stratification of race and net worth. The results, reflected in the table below, were telling. Wealthier patients, particularly those with a net worth of over US$1 million (millionaires), had notably lower diabetes rates and also tended to start GLP-1 therapy at lower BMIs than their less affluent counterparts. This difference was also clear when stratifying the millionaires by race. Among White/Other GLP-1 users, only 67% were diabetic. In contrast, millionaires, regardless of which other race, had much higher diabetes rates – an average of 75%.
Asian GLP-1 users had the highest diabetes rates across all income levels, with over 82% of patients being diabetic, regardless of net worth, as shown in the table below. This rate was significantly higher than that of other races, where diabetes prevalence was less pronounced across net worth levels.
“These demographic snapshots provide valuable insight into the types of patients accessing GLP-1 therapies, but they also raise deeper questions about healthcare access and equity. They highlight how certain socioeconomic factors intersect with health, revealing a complex landscape where race and wealth impact patient treatment and care.”
The cost of care: pre-GLP-1 medication spending and insulin usage among diabetes patients
When it comes to managing diabetes, patient out-of-pocket cost plays a significant role. Patients with the highest net worth spent the most on diabetes medications prior to starting GLP-1 therapy, shelling out between US$49 and US$65 per month, while those with the lowest net worth spent almost half that, between US$29 and US$39 per month.
Interestingly, as shown in the figure below, patients in the lowest net worth bracket were also far more likely to have relied on insulin before turning to GLP-1s.
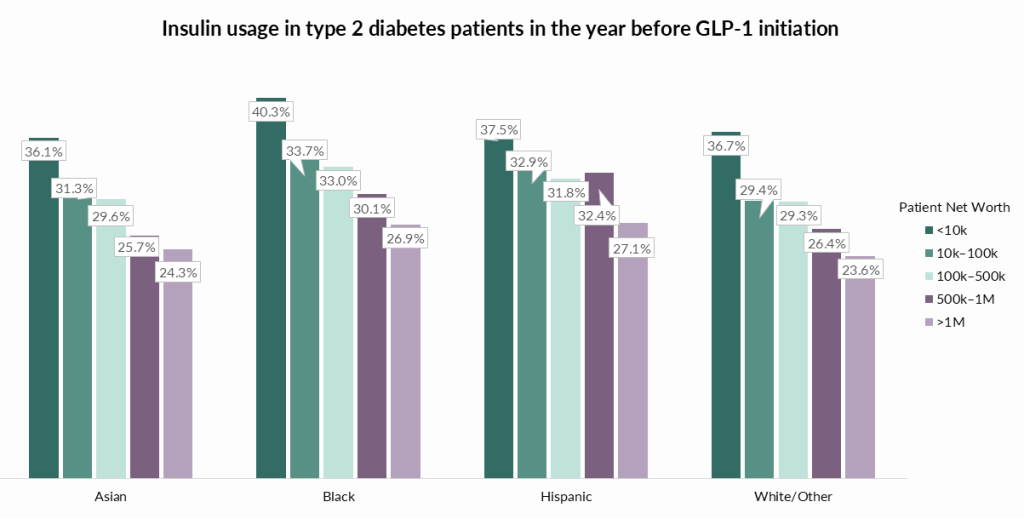
In fact, low-net-worth patients were 36% to 54% more likely to have used insulin compared to their wealthiest counterparts. This suggests that lower-net-worth individuals may have been managing their diabetes with more traditional medications before making the shift to GLP-1 therapies, possibly due to cost concerns or limited access to newer treatments.
“This disparity highlights how financial resources can influence both the type of care patients receive and their access to newer, potentially more effective treatments, as well as the timing of that care.”
Wealth versus weight: how BMI varies by and race in non-diabetic GLP-1 users
When it comes to non-diabetic patients using GLP-1s, the wealthiest individuals tend to start treatment with a lower BMI than those with lower net worth. Among millionaire Black patients, the median BMI before starting GLP-1s was 35.0, while for Black patients with a net worth under $10K, the median BMI was significantly higher at 39.4. That is a 13% difference, showing that less affluent patients are, on average, starting GLP-1 therapy at much higher BMIs. This trend is the same for the other race groups as well, where the wealthiest Asian and White/Other patients also had a 13% difference between them and the lowest net worth group. For Hispanic patients, the gap was slightly smaller, but still notable, with an 8% difference.
These findings point to the possibility that wealthier patients may have better access to preventative care, allowing them to start GLP-1 treatment earlier in their weight loss journey. Meanwhile, lower net worth individuals may delay starting GLP-1s until they reach a higher BMI and potentially worsening health conditions, likely due to financial barriers and/or reduced access to healthcare resources.
“This gap underscores the broader issue of healthcare inequality, where financial means can influence not only the timing of treatment but also its accessibility.”
Providing equitable access across all socioeconomic groups
Wealthier GLP-1 patients are less likely to be diabetic than their counterparts with lower net worths. Those non-diabetic millionaires also initiate GLP-1s at a 13% lower baseline BMI. While there are differences in the characteristics of the patients starting GLP-1s, there are not massive differences in the outcomes. This suggests that these differences in initiation are not because of expected outcome difference, but because the patients with a lower net worth have less ability to pay for the treatment or have less desire to take the medications.
The insights from our study reveal a critical aspect of health care: access to life-changing treatments is deeply influenced by socioeconomic factors. While the outcomes may not differ substantially between wealthy and less affluent patients, the disparities in who starts treatment (and when) are striking. Higher-net-worth individuals, with greater access to more resources, tend to begin GLP-1 therapies earlier and at a lower BMI, potentially reaping the benefits of preventative care sooner.
“Healthcare accessibility isn’t just about the availability of treatments, but also about affordability and timing of when patients can seek care. We believe that wealth should not dictate access to treatment, and these findings underscore the need for more inclusive approaches to treatment access.”
As GLP-1 therapies continue to be a viable option for both diabetes management and weight loss, ensuring equitable access for all socioeconomic groups will be vital in addressing broader health disparities.
Author
Michael Sicilia
RWD Data Scientist, Forian, Inc.

Michael Sicilia is a RWE Data Scientist at Forian, Inc., where he designs and conducts real-world evidence studies. Prior to joining Forian in June 2024, Michael was at EVERSANA where he implemented complex outcome, economic, burden-of-illness, and machine learning analyses on rare disease patient populations. In total, he has over 5 years of experience in the real-world data/evidence space and holds a bachelor’s degree in Computer Science.

Sponsorship for this Guest Column was provided by Forian.