Accelerating JCA readiness with an AI-enabled framework for early PICO identification
The EU Health Technology Assessment Regulation (EU HTAR) introduces the joint clinical assessment (JCA) to harmonize clinical evaluations across Member States. Central to this process is the PICO (population, intervention, comparator, outcomes) framework, yet defining and prioritizing multiple PICOs across national contexts is complex. As stakeholders reflect on early experiences from the Regulation’s first operational year, systematic PICO identification and prioritization have emerged as critical to optimizing evidence generation and submission readiness.
At ISPOR Europe 2025, researchers from Certara presented new work addressing this challenge. In their poster, “Early Systematic PICO Scenario Identification and Prioritization for EU HTA Joint Clinical Assessments,” Kurt Neeser, Elvira Müller, Dmitry Gultyaev, and Vishwas R Agashe from Evidence and Access at Certara introduce an integrated, evidence-based framework to systematically identify and prioritize PICO scenarios during early evidence planning and preparation for JCA submission. In this interview we speak with Kurt Neeser, Elvira Müller and Vishwas Agashe to learn more about their research and its implications for JCA preparedness.
Many thanks for speaking with The Evidence Base. Could you describe what motivated this research and the key challenges you sought to address for health technology developers, particularly when it comes to identifying and prioritizing PICO scenarios under the EU HTA framework and preparing for the tight 100-day JCA submission timeline?
One of the main challenges is that each EU Member State has its own healthcare system requirements and national HTA rules, which means manufacturers have to consider multiple PICO scenarios – all at once. When the final PICO scope for the JCA is released, developers have only about 100 days to prepare their submission, which simply isn’t enough time to conduct systematic literature reviews, manage the volume of studies, outcomes, and comparators involved in the required complex indirect treatment comparisons and network meta-analyses.
That’s why this work really must start long before those 100 days begin. In therapeutic areas like oncology, where treatment options have evolved over decades and the evidence base is vast, an early, systematic approach is essential. Our motivation was to help companies get ahead of that curve by identifying and prioritizing likely PICOs early in the process. Doing so not only supports timely evidence generation and indirect treatment comparisons but also helps inform future study designs by highlighting which outcomes and comparators will be most relevant across markets.
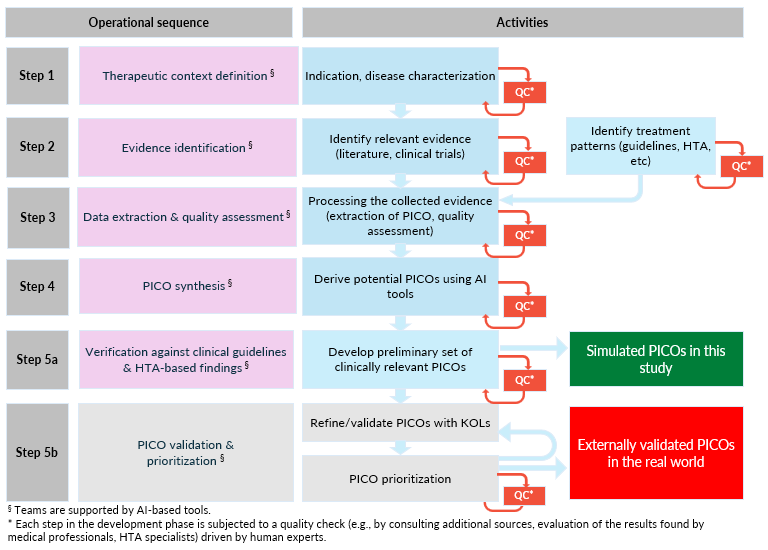
Your study presents an integrated, five-step framework and validation for systematic PICO identification and prioritization. Could you briefly walk us through these steps and explain how they work together to support JCA submission readiness?
Our framework helps health technology developers move from understanding the therapeutic context to final PICO prioritization. It starts by defining the disease area and current treatment landscape, then systematically searches in major databases and registries to capture relevant evidence. Next comes structured data extraction and quality assessment using standardized forms, followed by the development of PICO metrics that weight and rank potential scenarios based on their frequency and relevance. The final step is validation that brings in clinical, regulatory and payer experts to confirm that the prioritized PICOs align with published JCA guidance.
“Each step builds on the last to create a transparent, reproducible process that supports JCA submission readiness.”
What type of AI methods were used, and where did they add the most efficiency or value, particularly in automating evidence retrieval, curation, or PICO generation?
We used large language models like Google Gemini and ChatGPT 5, but that’s not really what makes this work unique – anyone can use those tools. What’s different here is the framework we built around them. The innovation isn’t the AI itself; it’s how Certara designed a structured, stepwise methodology that tells the AI exactly how to think about PICO generation in the context of the EU HTA framework. This proprietary AI-powered framework that we’re calling PICO Radar™ guides everything from defining the therapeutic landscape to ranking PICO scenarios and validating them against JCA requirements.
The AI adds the most value in automating the early, repetitive steps such as searching vast literature and registry data, extracting key study elements, and mapping them into standardized PICO matrices. That saves enormous amounts of time and ensures consistency. But the real intelligence comes from how those outputs feed into our ranking algorithms and validation steps, which bring in expert review to make sure the scenarios are clinically and regulatorily sound. In other words, the technology accelerates the process, but it’s the Certara framework that makes it reliable and decision ready.
A hypothetical new drug for type 2 diabetes was used to demonstrate your framework. What did this case study reveal about the scale, complexity, and practical feasibility of applying your methodology in real-world settings?
We tested our framework using a hypothetical new GIP/GLP-1 agonist in insulin-dependent type 2 diabetes (IDT2DM) to explore how it performs in a complex, data-rich therapeutic area. Diabetes was an ideal stress test for our methodology because of the sheer volume of available studies, comparators, and outcomes. In this exercise, focusing only on IDT2DM and on sources published within the last 5 years, we screened roughly 900 records across titles and abstracts and additional findings derived from trial registries. The AI-assisted workflow condensed that information efficiently, allowing us to focus on truly relevant evidence while maintaining transparency at each step.
“This case study demonstrated that our framework isn’t just a theoretical concept; it’s scalable and practical. Even in a crowded evidence space like diabetes, it handled the complexity of multiple treatment pathways, comparators, and endpoints without sacrificing scientific rigor.”
It also helped us refine the process further, confirming that the methodology can realistically support early PICO identification and prioritization across a range of therapeutic areas.
Finally, our PICO generation method underwent robust validation by applying it to scenarios in advanced hepatocellular carcinoma (aHCC) as outlined in the JCA scoping exercises published by the European Commission. Specifically, PICO Radar-generated scenarios were compared against published PICOs, with comparators normalized by drug class and outcomes mapped to standard HTA categories. This procedure revealed a high degree of agreement with HTA standards and provided valuable insights for refining the methodology, which will be implemented in subsequent steps and form the basis for the next generation of PICO Radar.
How does referencing national HTA guidance and disease-specific clinical guidelines help ensure that prioritized PICO scenarios remain relevant across different national contexts?
National HTA guidance and disease-specific clinical guidelines form the backbone of PICO generation. They define what’s considered standard of care in each country and shape the comparators and outcomes that will matter in an assessment. By referencing these sources early, our framework helps anticipate how different Member States might frame their PICOs and ensures that the scenarios we prioritize are grounded in real-world practice.
This step is especially important because health systems across Europe don’t always align. One country might emphasize a comparator that another barely considers. Incorporating national HTA and clinical guidance helps us reflect that diversity up front, so developers aren’t caught off guard later in the process. It’s a way of mimicking the reality of multi-country evidence requirements and maintaining relevance across all the markets that will ultimately review the JCA.
Looking ahead, how do you see this framework evolving? Could such an integrated, AI-supported approach become recognized as a best practice to support scientific advice under the EU HTAR?
We believe this framework has real potential to be recognized as a best practice because it brings transparency, speed, and consistency to an increasingly complex evidence landscape. As the volume of medical data continues to grow and timelines get shorter, tools that can structure and prioritize information efficiently will become essential for developers preparing for early scientific advice and JCAs.
That said, we’re very clear that automation doesn’t replace human expertise. Each step of our framework includes expert review and quality checks to make sure the AI outputs are accurate, relevant, and scientifically sound.
“The goal isn’t to remove people from the process but to give them better tools to focus on interpretation and decision-making rather than repetitive screening tasks.”
Looking ahead, we see this evolving beyond PICO generation towards automating treatment comparisons and supporting statistical analyses. Ultimately, it’s about equipping health technology developers with the insights they need, when they need them, to inform high-quality evidence generation and regulatory readiness.
Interviewees
Elvira Müller, PhD, MPH
Vice President, HTA Strategy and Access, Certara

Elvira Müller leads Certara’s HTA Strategy and Access practice in Europe, where she oversees evidence development and scientific consulting activities from the company’s German headquarters. With more than 20 years of experience in global market access and HTA, she has contributed to numerous European HTA engagements and collaborative EUnetHTA initiatives. Elvira is widely recognized for her expertise in JCA and Joint Scientific Consultation (JSC) processes, helping pharmaceutical clients align evidence generation with payer and regulatory expectations. Her leadership ensures the delivery of rigorous, high-quality scientific advice that maximizes the value of innovative medicines and medical technologies across diverse health systems.
Kurt Neeser, PhD, MPH
Senior Director, Evidence and Access, Certara

Kurt Neeser is a Senior Director within Certara’s Evidence and Access team in Germany, bringing over two decades of experience in HTA, health economics, and systematic evidence generation. He has led HTA and market access projects across Europe, the US and Asia, supporting pharmaceutical and medical device companies in developing robust value dossiers and economic evaluations. A published researcher and frequent international presenter, Kurt combines scientific rigor with practical insight to help clients navigate the evolving HTA landscape. He holds a PhD in Veterinary Medicine from the University of Bern (Switzerland) and a Master of Public Health jointly awarded by the Universities of Basel, Bern, and Zurich.
Vishwas Agashe, MSc
Associate Principal, Global Market Access, Pricing and Reimbursement, Certara

Vishwas Agashe is an Associate Principal in Certara’s Evidence and Access team based in the UK. He specializes in the design and implementation of global reimbursement and value demonstration strategies. With a strong foundation in life sciences and more than two decades of experience spanning academic research and strategic consulting, Vishwas helps pharmaceutical and medical device clients articulate product value to regulators, payers and providers. His work focuses on translating complex scientific data into actionable market access strategies that accelerate patient access to innovation. Vishwas is passionate about integrating evidence generation, pricing and payer insights to support successful launches across international markets. He holds a PhD in Molecular Biology and was a principal investigator and research group head in the Neuroscience program at the University of Oxford.
Acknowledgments
Special thanks to all authors of this research, Kurt Neeser, Elvira Müller, Dmitry Gultyaev, and Vishwas R Agashe from Evidence and Access at Certara.
Disclaimer
The opinions expressed in this feature are those of the author and do not necessarily reflect the views of The Evidence Base® or Becaris Publishing Ltd.
